













 8 / 12
8 / 12

Questions?
Call us at
(877) 668-1015
Visit
AlliantPlans.comContact your agent or broker
8
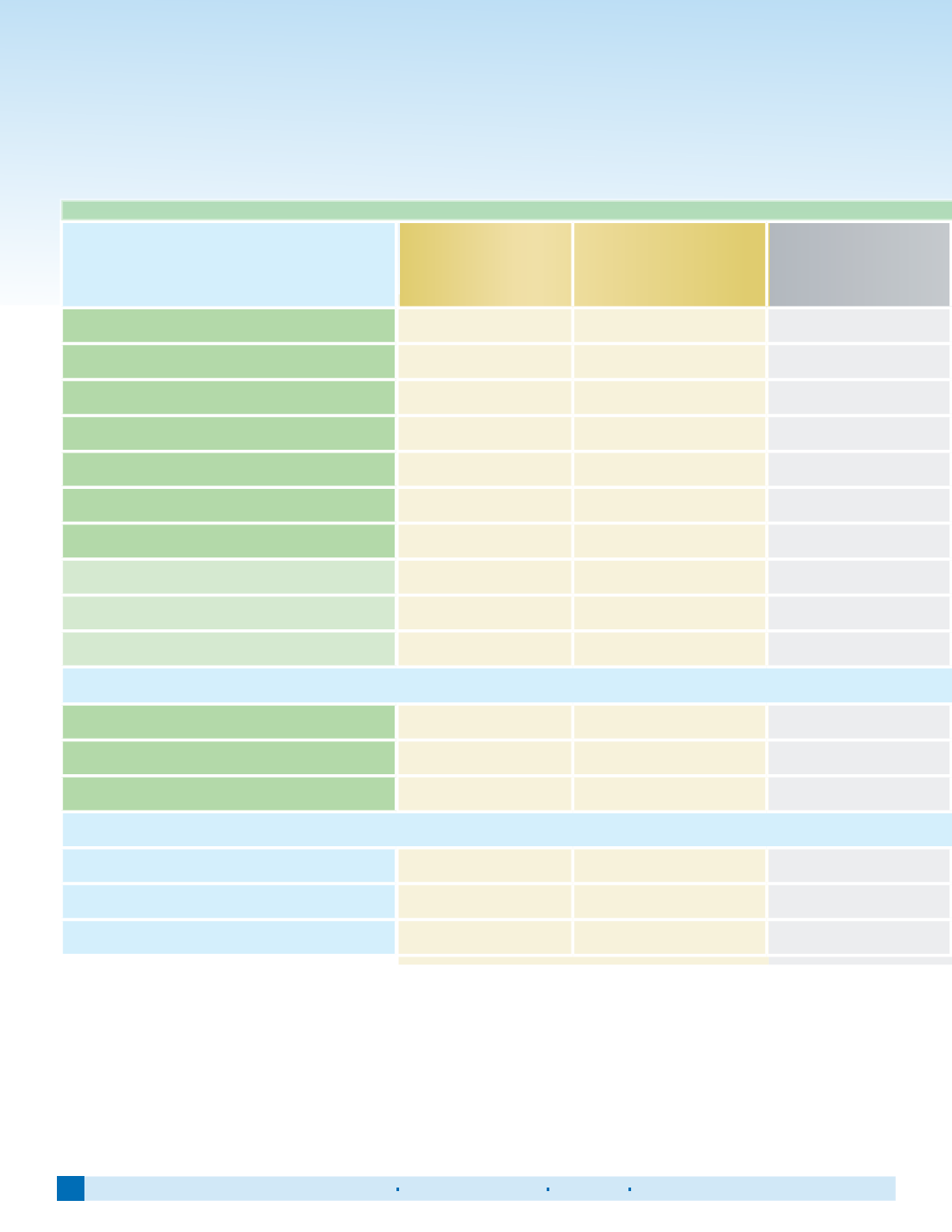
Compare our 60000 series plans
Plans available only OFF the Marketplace.
Plans have the Alliant network plus the PHCS network wrap.
IN-NETWORK BENEFITS
SoloCare
60023
Gold
SoloCare
60024
Gold
SoloCare
60028
Silver
Primary Care Physician Office Visit
$20 co-pay
$25 co-pay
$20 co-pay
Specialist Office Visit
$50 co-pay
$50 co-pay
$20 co-pay
Urgent Care
$75 co-pay
$75 co-pay
$75 co-pay
Out-Patient Mental/Behavioral Health
Out-Patient Rehabilitation
Skilled Nursing Facility
Emergency Room Visit
$250 co-pay
$300 co-pay
$250 co-pay
Co-insurance
(after deductible)
100%
90%
55%
Individual/Family Deductible
$3,000/ $6,000
$1,500/ $3,000
$1,850/ $3,700
Individual/Family Out-of-Pocket Maximum
$3,000/ $6,000
$3,500/ $7,000
$6,850/ $13,700
PRESCRIPTION DRUG BENEFITS
(after deductible)
Generic Drugs
$10
$10
$10
Preferred Brand Drugs
$35
$35
$35
Non-Preferred Brand & Specialty Drugs
$60
$60
$60
OUT-OF-NETWORK BENEFITS
Co-insurance
(after deductible)
60%
60%
30%
Individual/Family Deductible
$5,000/ $10,000
$5,000/ $10,000
$10,000/ $20,000
Individual/Family Out-of-Pocket Maximum
$10,000/ $20,000
$10,000/ $20,000
$15,000/ $30,000
- Out-of-pocket maximum includes deductible.
- Preventive Care Rx paid 100% - no cost-share for member.
- Plans are NOT HSA Compatible
- Blank cells indicate: subject to deductible and co-insurance